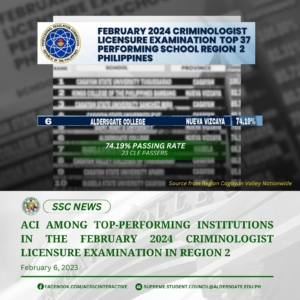
SSC NEWS | ALDERSGATE COLLEGE INC. RANKS 6 AMONG PERFORMING INSTITUTIONS IN THE FEBRUARY 2024 CRIMINOLOGIST LICENSURE EXAMINATION IN REGION 2
Aldersgate College Inc. is proud to announce that the February 2024 Criminologist Licensure Examination was one of the top-performing institutions with a passing rate of 74.19%. Congratulations to our new








